Pharmacologic Category: Selective Immunosuppressant.
Pharmacology: Pharmacodynamics: Mechanism of Action: Tofacitinib is a potent, selective inhibitor of the JAK family of kinases with a high degree of selectivity against other kinases in the human genome. In kinase assays, tofacitinib inhibits JAK1, JAK2, JAK3, and to a lesser extent TyK2. In cellular settings where JAK kinases signal in pairs, tofacitinib preferentially inhibits signaling by heterodimeric receptors associated with JAK3 and/or JAK1 with functional selectivity over receptors that signal via pairs of JAK2. Inhibition of JAK1 and JAK3 by tofacitinib blocks signaling through the common gamma chain-containing receptors for several cytokines, including IL-2, -4, -7, -9, -15, and -21. These cytokines are integral to lymphocyte activation, proliferation, and function and inhibition of their signaling may thus result in modulation of multiple aspects of the immune response. In addition, inhibition of JAK1 will result in attenuation of signaling by additional pro-inflammatory cytokines, such as IL-6 and Type I interferons. At higher exposures, inhibition of erythropoietin signaling could occur via inhibition of JAK2 signaling.
Pharmacodynamic Effect: In patients with rheumatoid arthritis, treatment up to 6 months with Tofacitinib (Xeljanz) was associated with dose-dependent reductions of circulating CD16/56+ natural killer (NK) cells, with estimated maximum reductions occurring at approximately 8-10 weeks after initiation of therapy. These changes generally resolved within 2-6 weeks after discontinuation of treatment. Treatment with Tofacitinib (Xeljanz) was associated with dose-dependent increases in B cell counts. Changes in circulating T-lymphocyte counts and T-lymphocyte subsets (CD3+, CD4+ and CD8+) were small and inconsistent.
Following long-term treatment (median duration of Tofacitinib (Xeljanz) treatment of approximately 5 years), CD4+ and CD8+ counts showed median reductions of 28% and 27%, respectively, from baseline. In contrast to the observed decrease after short-term dosing, CD16/56+ natural killer cell counts showed a median increase of 73% from baseline. CD19+ B cell counts showed no further increases after long-term Tofacitinib (Xeljanz) treatment. These changes returned toward baseline after temporary discontinuation of treatment. There was no evidence of an increased risk of serious or opportunistic infections or herpes zoster at low values of CD4+, CD8+ or NK cell counts or high B cell counts.
Changes in total serum IgG, IgM, and IgA levels over 6-month Tofacitinib (Xeljanz) dosing in patients with rheumatoid arthritis were small, not dose-dependent and similar to those seen on placebo.
After treatment with Tofacitinib (Xeljanz) in patients with rheumatoid arthritis, rapid decreases in serum C-reactive protein (CRP) were observed and maintained throughout dosing. Changes in CRP observed with Tofacitinib (Xeljanz) treatment do not reverse fully within 2 weeks after discontinuation, indicating a longer duration of pharmacodynamic activity compared to the half-life.
Clinical Safety: In one large randomized open-label PASS in RA patients who were 50 years or older with at least one additional cardiovascular risk factor and on a stable dose of methotrexate, patients were treated with tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily or a TNF inhibitor. Notably, in February 2019, the dose of tofacitinib in the 10 mg twice daily arm of the study was reduced to 5 mg twice daily after it was determined that the frequency of pulmonary embolism was increased in the tofacitinib 10 mg twice daily treatment arm versus the TNF inhibitor. Additionally, all-cause mortality was increased in the tofacitinib 10 mg twice daily treatment arm versus the TNF inhibitor and tofacitinib 5 mg twice daily treatment arms. In the final study data, patients in the tofacitinib 10 mg twice daily treatment arm were analyzed in their originally randomized treatment group. Results from final safety data from the study for selected events are as follows.
Mortality: The IRs (95% CI) for all-cause mortality for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.50 (0.33, 0.74), 0.80 (0.57, 1.09), 0.65 (0.50, 0.82), and 0.34 (0.20, 0.54) events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.49 (0.81, 2.74), 2.37 (1.34, 4.18), and 1.91 (1.12, 3.27), respectively.
The IRs (95% CI) for deaths associated with infection for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.08 (0.02, 0.20), 0.18 (0.08, 0.35), 0.13 (0.07, 0.22), and 0.06 (0.01, 0.17) events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.30 (0.29, 5.79), 3.10 (0.84, 11.45), and 2.17 (0.62, 7.62), respectively.
The IRs (95% CI) for deaths associated with cardiovascular events for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.25 (0.13, 0.43), 0.41 (0.25, 0.63), 0.33 (0.23, 0.46), and 0.20 (0.10, 0.36) events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.26 (0.55, 2.88), 2.05 (0.96, 4.39), and 1.65 (0.81, 3.34), respectively.
The IRs (95% CI) for deaths associated with malignancies for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.10 (0.03, 0.23), 0.00 (0.00, 0.08), 0.05 (0.02, 0.12), and 0.02 (0.00, 0.11) events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 4.88 (0.57, 41.74), 0 (0.00, Inf), and 2.53 (0.30, 21.64), respectively.
The IRs (95% CI) for deaths associated with other causes (excluding infections, cardiovascular events, malignancies) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.08 (0.02, 0.20), 0.21 (0.10, 0.38), 0.14 (0.08, 0.23), and 0.06 (0.01, 0.17) events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.30 (0.29, 5.81), 3.45 (0.95, 12.54), and 2.34 (0.67, 8.16), respectively.
In Tofacitinib (Xeljanz) clinical studies that included 10 mg twice a day, incidence rates for all-cause mortality in patients treated with Tofacitinib (Xeljanz) 10 mg twice a day have not been higher than rates in patients treated with Tofacitinib (Xeljanz) 5 mg twice a day. Mortality rates in patients treated with Tofacitinib (Xeljanz) are similar to those reported for patients with RA, PsO, PsA, pcJIA and UC, treated with biologic therapies.
Infections: The IRs (95% CI) for all infections for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 41.74 (39.21, 44.39), 48.73 (45.82, 51.77), 45.02 (43.10, 47.01), and 34.24 (32.07, 36.53) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.20 (1.10, 1.31), 1.36 (1.24, 1.49), and 1.28 (1.18, 1.38), respectively.
The IRs (95% CI) for serious infections for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 2.86 (2.41, 3.37), 3.64 (3.11, 4.23), 3.24 (2.89, 3.62), and 2.44 (2.02, 2.92) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.17 (0.92, 1.50), 1.48 (1.17, 1.87), and 1.32 (1.07, 1.63), respectively.
The IRs (95% CI) for opportunistic infections for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.76 (0.54, 1.04), 0.91 (0.66, 1.22), 0.84 (0.67, 1.04), and 0.42 (0.26, 0.64) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.82 (1.07, 3.09), 2.17 (1.29, 3.66), and 1.99 (1.23, 3.22), respectively. The majority of the opportunistic infections in the Tofacitinib (Xeljanz) treatment arms were opportunistic herpes zoster infections; a limited number of events with tuberculosis were also reported. Excluding opportunistic herpes zoster infections and tuberculosis, the IRs (95% CI) for all other opportunistic infections for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.08 (0.02, 0.20), 0.14 (0.06, 0.30), 0.11 (0.05, 0.20), and 0.06 (0.01, 0.17) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the hazard ratio (HR) (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.30 (0.29, 5.82), 2.40 (0.62, 9.29), and 1.84 (0.51, 6.59), respectively.
The IRs (95% CI) for herpes zoster (includes all herpes zoster events) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms) and TNF inhibitor were 3.75 (3.22, 4.34), 3.94 (3.38, 4.57), 3.84 (3.45, 4.26), and 1.18 (0.90, 1.52) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HR (95% CI) for herpes zoster with Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 3.17 (2.36, 4.27), 3.33 (2.48, 4.48), and 3.25 (2.46, 4.29), respectively.
Serious infections from non-interventional post approval safety study: Data from a non-interventional post approval safety study that evaluated tofacitinib in RA patients from a registry (US Corrona) showed that a numerically higher incidence rate of serious infection was observed for the 11 mg prolonged-release tablet administered once daily than the 5 mg film-coated tablet administered twice daily. Crude incidence rates (95% CI) (i.e., not adjusted for age or sex) from availability of each formulation at 12 months following initiation of treatment were 3.45 (1.93, 5.69) and 2.78 (1.74, 4.21) and at 36 months were 4.71 (3.08, 6.91) and 2.79 (2.01, 3.77) patients with events per 100 patient-years in the 11 mg prolonged-release tablet once daily and 5 mg film-coated tablet twice daily groups, respectively. The unadjusted hazard ratio was 1.30 (95% CI: 0.67, 2.50) at 12 months and 1.93 (95% CI: 1.15, 3.24) at 36 months for the 11 mg prolonged-release once daily dose compared to the 5 mg film-coated twice daily dose. Data is based on a small number of patients with events observed with relatively large confidence intervals and limited follow up time available in the 11 mg prolonged-release once daily dose group after 24 months.
Thromboembolism: Venous Thromboembolism: The IRs (95% CI) for VTE for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms) and TNF inhibitor were 0.33 (0.19, 0.53), 0.70 (0.49, 0.99), 0.51 (0.38, 0.67), and 0.20 (0.10, 0.37) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HR (95% CI) for VTE with Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.66 (0.76, 3.63), 3.52 (1.74, 7.12), and 2.56 (1.30, 5.05), respectively.
The IRs (95% CI) for PE for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms) and TNF inhibitor were 0.17 (0.08, 0.33), 0.50 (0.32, 0.74), 0.33 (0.23, 0.46), and 0.06 (0.01, 0.17) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HR (95% CI) for VTE with Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 2.93 (0.79, 10.83), 8.26 (2.49, 27.43), and 5.53 (1.70, 18.02), respectively.
The IRs (95% CI) for DVT for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms) and TNF inhibitor were 0.21 (0.11, 0.38), 0.31 (0.17, 0.51), 0.26 (0.17, 0.38), and 0.14 (0.06, 0.29) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HR (95% CI) for VTE with Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.54 (0.60, 3.97), 2.21 (0.90, 5.43), and 1.87 (0.81, 4.30), respectively.
In a post hoc exploratory biomarker analysis within a large randomized PASS in RA patients who were 50 years or older with at least one additional cardiovascular risk factor, occurrences of subsequent VTEs were observed more frequently in tofacitinib-treated patients with D-dimer level ≥2× ULN at 12 months treatment versus those with D-dimer level <2× ULN. This observation was not identified in TNFi-treated patients. Interpretation is limited by the low number of VTE events and restricted D-dimer test availability (only assessed at Baseline, Month 12, and at the end of the study). In patients who did not have a VTE during the study, mean D-dimer levels were significantly reduced at Month 12 relative to Baseline across all treatment arms. However, D-dimer levels ≥2× ULN at Month 12 were observed in approximately 30% of patients without subsequent VTE events, indicating limited specificity of D-dimer testing in this study. Considering the data and the overall limitations of this post hoc exploratory biomarker analysis, there is limited utility of conducting D-dimer monitoring in the context of risk mitigation for VTE events.
Arterial Thromboembolism: The IRs (95% CI) for arterial thromboembolism (ATE) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms) and TNF inhibitor were 0.92 (0.68, 1.22), 0.94 (0.68, 1.25), 0.93 (0.75, 1.14), and 0.82 (0.59, 1.12) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HR (95% CI) for ATE with Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.12 (0.74, 1.70), 1.14 (0.75, 1.74), and 1.13 (0.78, 1.63), respectively.
Major Adverse Cardiovascular Events (MACE), Including Myocardial Infarction: MACE includes non fatal myocardial infarction, non fatal stroke, and cardiovascular deaths excluding fatal pulmonary embolism. The IRs (95% CI) for MACE for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.91 (0.67, 1.21), 1.05 (0.78, 1.38), 0.98 (0.79, 1.19), and 0.73 (0.52, 1.01) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.24 (0.81, 1.91), 1.43 (0.94, 2.18), and 1.33 (0.91, 1.94), respectively.
In the Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz), and TNFi treatment arms, there were a total of 19, 19, 38, and 11 patients with MI events, respectively. Of these totals, the number of patients with fatal MI events was 0, 3, 3, and 3, respectively, whereas the number of patients with non-fatal MI events was 19, 16, 35, and 8, respectively. Therefore, the IRs that follow are for non-fatal MI. The IRs (95% CI) for non-fatal MI for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.37 (0.22, 0.57), 0.33 (0.19, 0.53), 0.35 (0.24, 0.48), and 0.16 (0.07, 0.31) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 2.32 (1.02, 5.30), 2.08 (0.89, 4.86), and 2.20 (1.02, 4.75), respectively.
Malignancies Excluding NMSC: The IRs (95% CI) for malignancies excluding NMSC for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 1.13 (0.87, 1.45), 1.13 (0.86, 1.45), 1.13 (0.94, 1.35), and 0.77 (0.55, 1.04) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.47 (1.00, 2.18), 1.48 (1.00, 2.19), and 1.48 (1.04, 2.09), respectively.
The IRs (95% CI) for lymphoma for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.07 (0.02, 0.18), 0.11 (0.04, 0.24), 0.09 (0.04, 0.17), and 0.02 (0.00, 0.10) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 3.99 (0.45, 35.70), 6.24 (0.75, 51.86), and 5.09 (0.65, 39.78), respectively.
The IRs (95% CI) for lung cancer for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.23 (0.12, 0.40), 0.32 (0.18, 0.51), 0.28 (0.19, 0.39), and 0.13 (0.05, 0.26) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.84 (0.74, 4.62), 2.50 (1.04, 6.02), and 2.17 (0.95, 4.93), respectively.
NMSC: The IRs (95% CI) for NMSC for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.61 (0.41, 0.86), 0.69 (0.47, 0.96), 0.64 (0.50, 0.82), and 0.32 (0.18, 0.52) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.90 (1.04, 3.47), 2.16 (1.19, 3.92), and 2.02 (1.17, 3.50), respectively.
The IRs (95% CI) for basal cell carcinoma for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.37 (0.22, 0.58), 0.33 (0.19, 0.54), 0.35 (0.24, 0.49), and 0.26 (0.14, 0.44) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.43 (0.71, 2.90), 1.28 (0.61, 2.66), and 1.36 (0.72, 2.56), respectively.
The IRs (95% CI) for cutaneous squamous cell carcinoma for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.29 (0.16, 0.48), 0.45 (0.29, 0.69), 0.37 (0.26, 0.51), and 0.16 (0.07, 0.31) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.82 (0.77, 4.30), 2.86 (1.27, 6.43), and 2.32 (1.08, 4.99), respectively.
Gastrointestinal Perforations: The IRs (95% CI) for gastrointestinal perforations for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 0.17 (0.08, 0.33), 0.10 (0.03, 0.24), 0.14 (0.08, 0.23), and 0.08 (0.02, 0.20) patients with events per 100 PYs, respectively. Compared with TNF inhibitor, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 2.20 (0.68, 7.15), 1.29 (0.35, 4.80), and 1.76 (0.58, 5.34), respectively.
Fractures: The IRs (95% CI) for fractures for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, all Tofacitinib (Xeljanz) (combines 5 mg twice daily and 10 mg twice daily treatment arms), and TNF inhibitor were 2.79 (2.34, 3.30), 2.87 (2.40, 3.40), 2.83 (2.50, 3.19) and 2.27 (1.87, 2.74) patients with events per 100 PYs respectively. Compared with TNFi, the HRs (95% CI) for Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and all Tofacitinib (Xeljanz) were 1.23 (0.96, 1.58) 1.26 (0.97, 1.62) and 1.24 (0.99, 1.55) respectively.
Laboratory tests: Liver enzyme tests: The percentages of patients with at least one post-baseline ALT elevation >1x ULN, 3x ULN, and 5x ULN for the Tofacitinib (Xeljanz) 5 mg twice daily treatment arm were 52.83, 6.01, and 1.68, respectively. The percentages for the Tofacitinib (Xeljanz) 10 mg twice daily treatment arm were 54.46, 6.54, and 1.97, respectively. The percentages for all Tofacitinib (Xeljanz) (combines Tofacitinib (Xeljanz) 5 mg twice daily and Tofacitinib (Xeljanz) 10 mg twice daily) were 53.64, 6.27, and 1.82, respectively. The percentages for the TNF inhibitor treatment arm were 43.33, 3.77, and 1.12, respectively.
The percentages of patients with at least one post-baseline AST elevation >1x ULN, 3x ULN, and 5x ULN for the Tofacitinib (Xeljanz) 5 mg twice daily treatment arm were 45.84, 3.21, and 0.98, respectively. The percentages for the Tofacitinib (Xeljanz) 10 mg twice daily treatment arm were 51.58, 4.57, and 1.62, respectively. The percentages for all Tofacitinib (Xeljanz) (combines Tofacitinib (Xeljanz) 5 mg twice daily and Tofacitinib (Xeljanz) 10 mg twice daily) were 48.70, 3.89, and 1.30, respectively. The percentages for the TNF inhibitor treatment arm were 37.18, 2.38, and 0.70, respectively.
Lipids: At 12 months, in the Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and TNF inhibitor treatment arms, the mean percent increase in LDL cholesterol was 13.80, 17.04, and 5.50, respectively. At 24 months, the mean percent increase was 12.71, 18.14, and 3.64, respectively.
At 12 months, in the Tofacitinib (Xeljanz) 5 mg twice daily, Tofacitinib (Xeljanz) 10 mg twice daily, and TNF inhibitor treatment arms, the mean percent increase in HDL cholesterol was 11.71, 13.63, and 2.82, respectively. At 24 months, the mean percent increase was 11.58, 13.54, and 1.42, respectively.
Clinical Efficacy: Rheumatoid Arthritis: Tofacitinib (Xeljanz XR) 11 mg once daily has demonstrated pharmacokinetic equivalence (AUC and C
max) to Tofacitinib (Xeljanz) 5 mg twice daily. The recommended dose of Tofacitinib (Xeljanz XR) is 11 mg once daily. All information provided in this section is applicable to Tofacitinib (Xeljanz XR).
The efficacy and safety of Tofacitinib (Xeljanz) were assessed in six randomized, double-blind, controlled multicenter studies in patients >18 years with active rheumatoid arthritis diagnosed according to American College of Rheumatology (ACR) criteria. Patients had at least 6 tender and 6 swollen joints at randomization (4 swollen and tender joints for Study II). Tofacitinib (Xeljanz), 5 or 10 mg twice daily, was given as monotherapy (Study I) and in combination with DMARDs (Study II) in patients with an inadequate response to those drugs, and in combination with MTX in patients with either an inadequate response to MTX (Studies III and Study IV) or inadequate efficacy or lack of tolerance to at least one approved TNF-inhibiting biologic agent (Study V).
Study I was a 6-month monotherapy study in which 610 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to a DMARD (non-biologic or biologic) received Tofacitinib (Xeljanz) 5 or 10 mg twice daily or placebo. At the Month 3 visit, all patients randomized to placebo treatment were advanced in a blinded fashion to a second predetermined treatment of Tofacitinib (Xeljanz) 5 or 10 mg twice daily. The primary endpoints at Month 3 were the proportion of patients who achieved an ACR20 response, changes in Health Assessment Questionnaire - Disability Index (HAQ-DI), and rates of Disease Activity Score DAS28-4 (ESR) <2.6.
Study II was a 12-month study in which 792 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to a non-biologic DMARD received Tofacitinib (Xeljanz) 5 or 10 mg twice daily or placebo added to background DMARD treatment (excluding potent immunosuppressive treatments such as azathioprine or cyclosporine). At the Month 3 visit, non-responding patients randomized to placebo treatment were advanced in a blinded fashion to a second predetermined treatment of Tofacitinib (Xeljanz) 5 or 10 mg twice daily. At the end of Month 6, all placebo patients were advanced to their second predetermined treatment in a blinded fashion. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, changes in HAQ-DI at Month 3 and rates of DAS28-4(ESR) <2.6 at Month 6.
Study III was a 12-month study in which 717 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to MTX. Patients received Tofacitinib (Xeljanz) 5 or 10 mg twice daily, adalimumab 40 mg subcutaneously every other week, or placebo added to background MTX. Placebo patients were advanced as in Study II. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, HAQ-DI at Month 3, and DAS28-4(ESR) <2.6 at Month 6.
Study IV was a 2-year study with a planned analysis at 1 year in which 797 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to MTX received Tofacitinib (Xeljanz) 5 or 10 mg twice daily or placebo added to background MTX. Placebo patients were advanced as in Study II. The primary endpoints were the proportion of patients who achieved an ACR20 response at Month 6, mean change from baseline in van der Heijde-modified total Sharp Score (mTSS) at Month 6, HAQ-DI at Month 3, and DAS28-4(ESR) <2.6 at Month 6.
Study V was a 6-month study in which 399 patients with moderate to severe active rheumatoid arthritis who had an inadequate response to at least one approved TNF-inhibiting biologic agent received Tofacitinib (Xeljanz) 5 or 10 mg twice daily or placebo added to background MTX. At the Month 3 visit, all patients randomized to placebo treatment were advanced in a blinded fashion to a second predetermined treatment of Tofacitinib (Xeljanz) 5 or 10 mg twice daily. The primary endpoints at Month 3 were the proportion of patients who achieved an ACR20 response, HAQ-DI, and DAS28-4(ESR) <2.6.
Study VI was a 2-year monotherapy study with a planned analysis at 1 year in which 952 MTX-naïve patients with moderate to severe active rheumatoid arthritis received Tofacitinib (Xeljanz) 5 or 10 mg twice daily or MTX dose-titrated over 8 weeks from 10 to 20 mg weekly. The primary endpoints were mean change from baseline in van der Heijde mTSS at Month 6 and the proportion of patients who achieved an ACR70 response at Month 6.
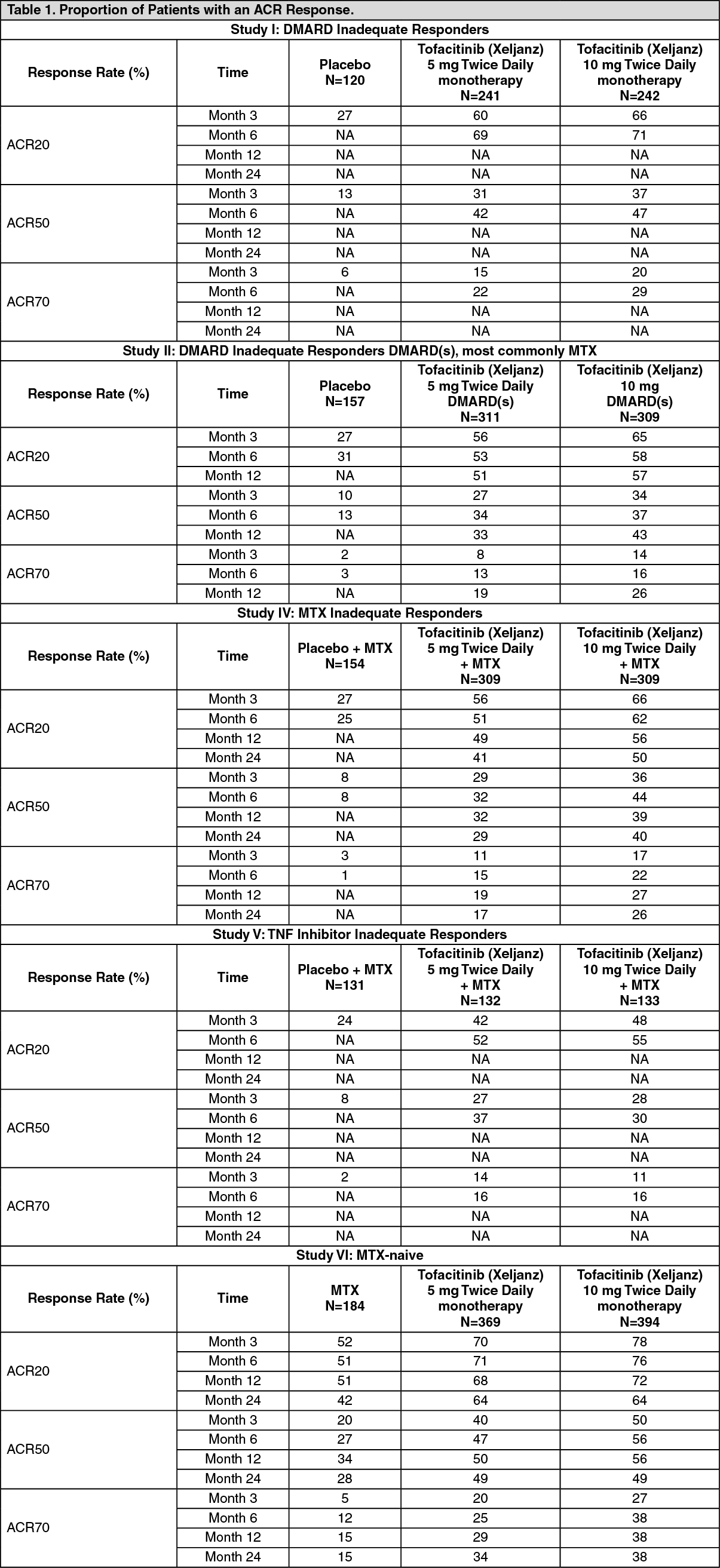
Clinical Response: ACR Response: The percentages of Tofacitinib (Xeljanz)-treated patients achieving ACR20, ACR50 and ACR70 responses in Studies I, II, IV, V and VI are shown in Table 1. In all studies, patients treated with either 5 or 10 mg twice daily Tofacitinib (Xeljanz) had statistically significant ACR20, ACR50 and ACR70 response rates at Month 3 and Month 6 vs. placebo (or vs. MTX in Study VI) treated patients.
In Study IV, ACR20/50/70 response rates at Month 12 were maintained through Month 24.
In Study VI (Table 1), the difference from MTX in both tofacitinib groups, in achieving ACR20, ACR50 and ACR70 response rates was statistically significant at all timepoints (p ≤0.0001). Tofacitinib, administered as monotherapy in MTX-naïve patients, significantly improved RA signs and symptoms in comparison to MTX. Efficacy observed with tofacitinib was sustained through Month 24.
In Studies I, II, and V, improvement in ACR20 response rate vs. placebo was observed within 2 weeks.
During the 3 month (Studies I and V) and 6 month (Studies II, III, and IV) controlled portions of the studies, patients treated with Tofacitinib (Xeljanz) at a dose of 10 mg twice daily generally had higher response rates compared to patients treated with Tofacitinib (Xeljanz) 5 mg twice daily. In Study III, the primary endpoints were the proportion achieving an ACR20 response at Month 6; change in HAQ-DI at Month 3, and DAS28-4(ESR) <2.6 at Month 6. The data for these primary outcomes were 51.5, 52.6, 47.2 and 28.3%; -0.55, -0.61, -0.49 and -0.24; and 6.2%, 12.5%, 6.7% and 1.1% for the 5 mg twice daily Tofacitinib (Xeljanz), 10 mg twice daily Tofacitinib (Xeljanz), adalimumab 40 mg subcutaneously every other week and placebo groups, respectively. For a pre-specified secondary endpoint, the ACR70 response rates at Month 6 for the 5 mg twice daily and 10 mg twice daily Tofacitinib (Xeljanz) groups were significantly greater than adalimumab 19.9%, 21.9% and 9.1%, respectively.
The treatment effect was similar in patients independent of rheumatoid factor status, age, gender, race, or disease status. Time to onset was rapid (as early as Week 2 in Studies I, II and V) and the magnitude of response continued to improve with duration of treatment. As with the overall ACR response in patients treated with 5 mg or 10 mg twice daily Tofacitinib (Xeljanz), each of the components of the ACR response was consistently improved from baseline including: tender and swollen joint counts; patient and physician global assessment; disability index scores; pain assessment and CRP compared to patients receiving placebo plus MTX or other DMARDs in all studies.
DAS28-4(ESR) Response: Patients in the Phase 3 studies had a mean Disease Activity Score (DAS28-4[ESR]) of 6.1-6.7 at baseline. Significant reductions in DAS28-4(ESR) from baseline (mean improvement) of 1.8-2.0 and 1.9-2.2 were observed in 5 mg and 10 mg Tofacitinib (Xeljanz)-treated patients, respectively, compared to placebo-treated patients (0.7-1.1) at 3 Months. The proportion of patients achieving a DAS28 clinical remission (DAS28-4(ESR) <2.6) in Studies II, III and IV was significantly higher in patients receiving 5 mg or 10 mg tofacitinib (6%-9% and 13%-16%, respectively) compared to 1%-3% of placebo patients at 6 months. In Study III, the percentages of patients achieving DAS28-4(ESR) <2.6 observed for Tofacitinib (Xeljanz) 5 mg twice daily, 10 mg twice daily, and adalimumab at Month 6 were 6.2%, 12.5%, and 6.7%, respectively.
In a pooled analysis of the Phase 3 studies, the 10 mg twice daily dose provided increased benefit over the 5 mg twice daily dose in multiple measures of signs and symptoms: improvement from baseline (ACR20, ACR50, and ACR70 response rates), and achievement of targeted disease activity state (either DAS28-4(ESR) <2.6 or ≤3.2). Greater benefits of 10 mg versus 5 mg were shown in the more stringent measures (i.e., ACR70 and DAS28-4 (ESR) <2.6 response rates). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The results of the proportion of patients with an ACR Response for Studies I, II, IV, V and VI are shown in Table 1. Similar results were observed in Study III.
The results of the components of the ACR response criteria for Studies IV and V are shown in Table 2. Similar results were observed in Studies I, II and III. (See Table 2.)
Click on icon to see table/diagram/image
The percent of ACR20 responders by visit for Study IV is shown in Figure 1. Similar responses were observed in Studies I, II, III and V. (See Figure 1.)
Click on icon to see table/diagram/image
Radiographic Response: Two studies were conducted to evaluate the effect of Tofacitinib (Xeljanz) on structural joint damage. In Study IV and Study VI, inhibition of progression of structural joint damage was assessed radiographically and expressed as mean change from baseline in mTSS and its components, the erosion score and joint space narrowing (JSN) score, at Months 6 and 12. The proportion of patients with no radiographic progression (mTSS change less than or equal to 0.5) was also assessed.
In Study IV, Tofacitinib (Xeljanz) 10 mg twice daily plus background MTX resulted in significantly greater inhibition of the progression of structural damage compared to placebo plus MTX at Months 6 and 12. When given at a dose of 5 mg twice daily, Tofacitinib (Xeljanz) plus MTX exhibited similar effects on mean progression of structural damage (not statistically significant). Analysis on erosion and JSN score were consistent with overall results. These results are shown in Table 3.
In the placebo plus MTX group, 78% of patients experienced no radiographic progression at Month 6 compared to 89% and 87% of patients treated with Tofacitinib (Xeljanz) 5 or 10 mg twice daily respectively, plus MTX, both significant vs. placebo plus MTX. (See Table 3.)
Click on icon to see table/diagram/image
In Study VI, Tofacitinib (Xeljanz) monotherapy resulted in significantly greater inhibition of the progression of structural damage compared to MTX at Months 6 and 12 as shown in Table 4, which was also maintained at Month 24. Analyses of erosion and JSN scores were consistent with overall results.
In the MTX group, 70% of patients experienced no radiographic progression at Month 6 compared to 84% and 90% of patients treated with tofacitinib 5 or 10 mg twice daily respectively, both significant vs. MTX. (See Table 4.)
Click on icon to see table/diagram/image
Physical Function Response and Health Related Outcomes: Improvement in physical functioning was measured by the HAQ-DI. Patients receiving Tofacitinib (Xeljanz) 5 or 10 mg twice daily demonstrated significantly greater improvement from baseline in physical functioning compared to placebo at Month 3 (Studies I, II, III, and V) and Month 6 (Studies II and III). Tofacitinib (Xeljanz) 5 or 10 mg twice daily-treated patients exhibited significantly greater improved physical functioning compared to placebo as early as Week 2 in Studies I and II. In Study III, mean HAQ-DI improvements were maintained to 12 months in Tofacitinib (Xeljanz)-treated patients. Mean HAQ-DI improvements were maintained for 36 months in the ongoing open-label extension studies. Compared with adalimumab-treated patients, at Month 3, patients in the Tofacitinib (Xeljanz) 5 mg twice daily had similar decreases from baseline in HAQ-DI values and patients in 10 mg twice daily group had significantly greater decreases in HAQ-DI. The mean change in HAQ-DI from baseline to Month 3 in Studies I to VI are shown in Table 5. (See Table 5.)
Click on icon to see table/diagram/image
Health-related quality of life was assessed by the Short Form Health Survey (SF-36) in all 5 studies. In these studies, patients receiving Tofacitinib (Xeljanz) 10 mg twice daily demonstrated significantly greater improvement from baseline compared to placebo in all 8 domains of the SF-36 as well as the Physical Component Summary (PCS) and the Mental Component Summary (MCS) at Month 3. Both Tofacitinib (Xeljanz)-treated groups exhibited significantly greater improvement from baseline compared to placebo in all 8 domains as well as PCS and MCS at Month 3 in Studies I, IV, and V. In Studies III and IV, mean SF-36 improvements were maintained to 12 months in Tofacitinib (Xeljanz)-treated patients.
Improvement in fatigue was evaluated by the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale at Month 3 in all studies. Patients receiving Tofacitinib (Xeljanz) 5 or 10 mg twice daily demonstrated significantly greater improvement from baseline in fatigue compared to placebo in all 5 studies. In Studies III and IV, mean FACIT-F improvements were maintained to 12 months in Tofacitinib (Xeljanz)-treated patients.
Improvement in sleep was assessed using the Sleep Problems Index I and II summary scales of the Medical Outcomes Study Sleep (MOS-Sleep) measure at Month 3 in all studies. Patients receiving Tofacitinib (Xeljanz) 5 or 10 mg twice daily demonstrated significantly greater improvement from baseline in both scales compared to placebo in Studies II, III, and IV. In Studies III and IV, mean improvements in both scales were maintained to 12 months in Tofacitinib (Xeljanz)-treated patients.
Improvement in productivity was evaluated using the Work Limitations Questionnaire (WLQ) scale at Month 3 in all studies. Patients receiving Tofacitinib (Xeljanz) 10 mg twice daily demonstrated significantly greater improvement from baseline in the Overall Output Summary Scale compared to placebo in Studies III, IV, and V. In Studies III and IV, mean Overall Output improvements were maintained to 12 months in Tofacitinib (Xeljanz) 10 mg twice daily-treated patients.
Durability of clinical responses: Durability of effect was assessed by ACR20, ACR50, ACR70 response rates, mean HAQ-DI, and mean DAS28-4(ESR) in the three Phase 3 DMARD IR studies with duration of at least one year. Efficacy was maintained in all tofacitinib treatment groups through to the end of the studies. Evidence of persistence of efficacy with tofacitinib treatment for up to 6 years is also provided from data in a large randomized PASS in RA patients 50 years and older with at least one additional CV risk factor, as well as in completed open-label, long-term follow-up studies up to 8 years.
Pharmacokinetics: Tofacitinib (Xeljanz): The PK profile of Tofacitinib (Xeljanz) is characterized by rapid absorption (peak plasma concentrations are reached within 0.5-1 hour), rapid elimination (half-life of ~3 hours) and dose-proportional increases in systemic exposure. Steady-state concentrations are achieved in 24-48 hours with negligible accumulation after twice daily administration.
Tofacitinib (Xeljanz XR): Following oral administration of Tofacitinib (Xeljanz XR), peak plasma concentrations are reached at 4 hours and half-life is about 6 to 8 hours. Steady state concentrations are achieved within 48 hours with negligible accumulation after once daily administration. AUC and C
max of tofacitinib for Xeljanz XR 11 mg administered once daily are bioequivalent to those of Tofacitinib (Xeljanz) 5 mg administered twice daily.
Absorption and Distribution: Tofacitinib is well-absorbed, with an oral bioavailability of 74% following administration of Tofacitinib (Xeljanz). Co-administration of Tofacitinib (Xeljanz) with a high-fat meal resulted in no changes in AUC while C
max was reduced by 32%. In clinical trials, tofacitinib was administered without regard to meal.
After intravenous administration, the volume of distribution is 87 L. Approximately 40% of circulating tofacitinib is bound to proteins. Tofacitinib binds predominantly to albumin and does not appear to bind to α1-acid glycoprotein. Tofacitinib distributes equally between red blood cells and plasma.
Tofacitinib (Xeljanz XR): Co-administration of Tofacitinib (Xeljanz XR) with a high-fat meal resulted in no changes in AUC while C
max was increased by 27% and T
max was extended by approximately 1 hour.
Metabolism and Elimination: Clearance mechanisms for tofacitinib are approximately 70% hepatic metabolism and 30% renal excretion of the parent drug. The metabolism of tofacitinib is primarily mediated by CYP3A4 with minor contribution from CYP2C19. In a human radiolabeled study, more than 65% of the total circulating radioactivity was accounted for by unchanged drug, with the remaining 35% attributed to 8 metabolites, each accounting for less than 8% of total radioactivity. All metabolites have been observed in animal species and are predicted to have ≤10% of the potency of tofacitinib for JAK1/3 inhibition. No evidence of stereo conversion in human samples was detected. The pharmacologic activity of tofacitinib is attributed to the parent molecule.
In vitro, tofacitinib is a substrate for multidrug resistance (MDR) 1, but not for breast cancer resistance protein (BCRP), organic anion transporting polypeptide (OATP) 1B1/1B3, or organic cationic transporter (OCT) 1/2, and is not an inhibitor of MDR1, OAT P1B1/1B3, OCT2, organic anion transporter (OAT) 1/3, or multidrug resistance-associated protein (MRP) at clinically meaningful concentrations.
Pharmacokinetic data and dosing recommendations for special populations and drug interactions are provided in Figure 2.
Modifications required for special populations are described in Dosage & Administration.
Pharmacokinetics in RA Patients: Population PK analysis in rheumatoid arthritis patients indicated that systemic exposure (AUC) of tofacitinib in the extremes of body weight (40 kg, 140 kg) were similar to that of a 70 kg patient. Elderly patients 80 years of age were estimated to have <5% higher AUC relative to the mean age of 55 years. Women were estimated to have 7% lower AUC compared to men. The available data have also shown that there are no major differences in tofacitinib AUC between White, Black and Asian patients. An approximate linear relationship between body weight and volume of distribution was observed, resulting in higher peak (C
max) and lower trough (C
min) concentrations in lighter patients. However, this difference is not considered to be clinically relevant. The between-subject variability (percentage coefficient of variation) in AUC of Tofacitinib (Xeljanz) is estimated to be approximately 27%.
Renal Impairment: Patients with mild, moderate, and severe renal impairment had 37%, 43% and 123% higher AUC, respectively, compared with healthy patients (see Dosage & Administration). In patients with end-stage renal disease, the contribution of dialysis to the total clearance of tofacitinib was relatively small.
Hepatic Impairment: Patients with mild and moderate hepatic impairment had 3% and 65% higher AUC, respectively, compared with healthy patients. Patients with severe hepatic impairment were not studied (see Dosage & Administration).
Pediatric Population: The pharmacokinetics, safety and efficacy of Tofacitinib in pediatric patients have not been established for rheumatoid arthritis. (See Figure 2.)
Click on icon to see table/diagram/image
Toxicology: Preclinical Safety Data: In non-clinical studies, effects were observed on the immune and hematopoietic systems that were attributed to the pharmacological properties (JAK inhibition) of tofacitinib. Secondary effects from immunosuppression, such as bacterial and viral infections and lymphoma were observed at clinically relevant doses. Other findings at doses well above human exposures included effects on the liver, lung and gastrointestinal systems.
Lymphoma was observed in 3 of 8 adult and 0 of 14 juvenile monkeys dosed with tofacitinib at 5 mg/kg twice daily. The no observed adverse effect level (NOAEL) for the lymphomas was 1 mg/kg twice daily. The unbound AUC at 1 mg/kg twice daily was 341 ng·h/mL, which is approximately half of the unbound AUC at 10 mg twice daily and similar to the unbound AUC at 5 mg twice daily in humans.
Tofacitinib is not mutagenic or genotoxic based on the results of a series of
in vitro and
in vivo tests for gene mutations and chromosomal aberrations.
The carcinogenic potential of tofacitinib was assessed in 6-month rasH2 transgenic mouse carcinogenicity and 2-year rat carcinogenicity studies. Tofacitinib was not carcinogenic in mice up to a high dose of 200 mg/kg/day (unbound drug AUC of ~19-fold the human AUC at 10 mg twice daily). Benign Leydig cell tumors were observed in rats: benign Leydig cell tumors in rats are not associated with a risk of Leydig cell tumors in humans. Hibernomas (malignancy of brown adipose tissue) were observed in female rats at doses ≥30 mg/kg/day (unbound drug AUC of ~41-fold the human AUC at 10 mg twice daily). Benign thymomas were observed in female rats dosed only at the 100 reduced to 75 mg/kg/day dose (unbound drug AUC of ~94-fold the human AUC at 10 mg twice daily).
Tofacitinib was shown to be teratogenic in rats and rabbits, and have effects in rats on female fertility, parturition, and peri-/post-natal development. Tofacitinib had no effects on male fertility, sperm motility, or sperm concentration. Tofacitinib was secreted in milk of lactating rats. In studies conducted in juvenile rats and monkeys tofacitinib-related effects on the immune system were similar to those in adult animals. There were no tofacitinib-related effects on reproductive system or bone development in males or females.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image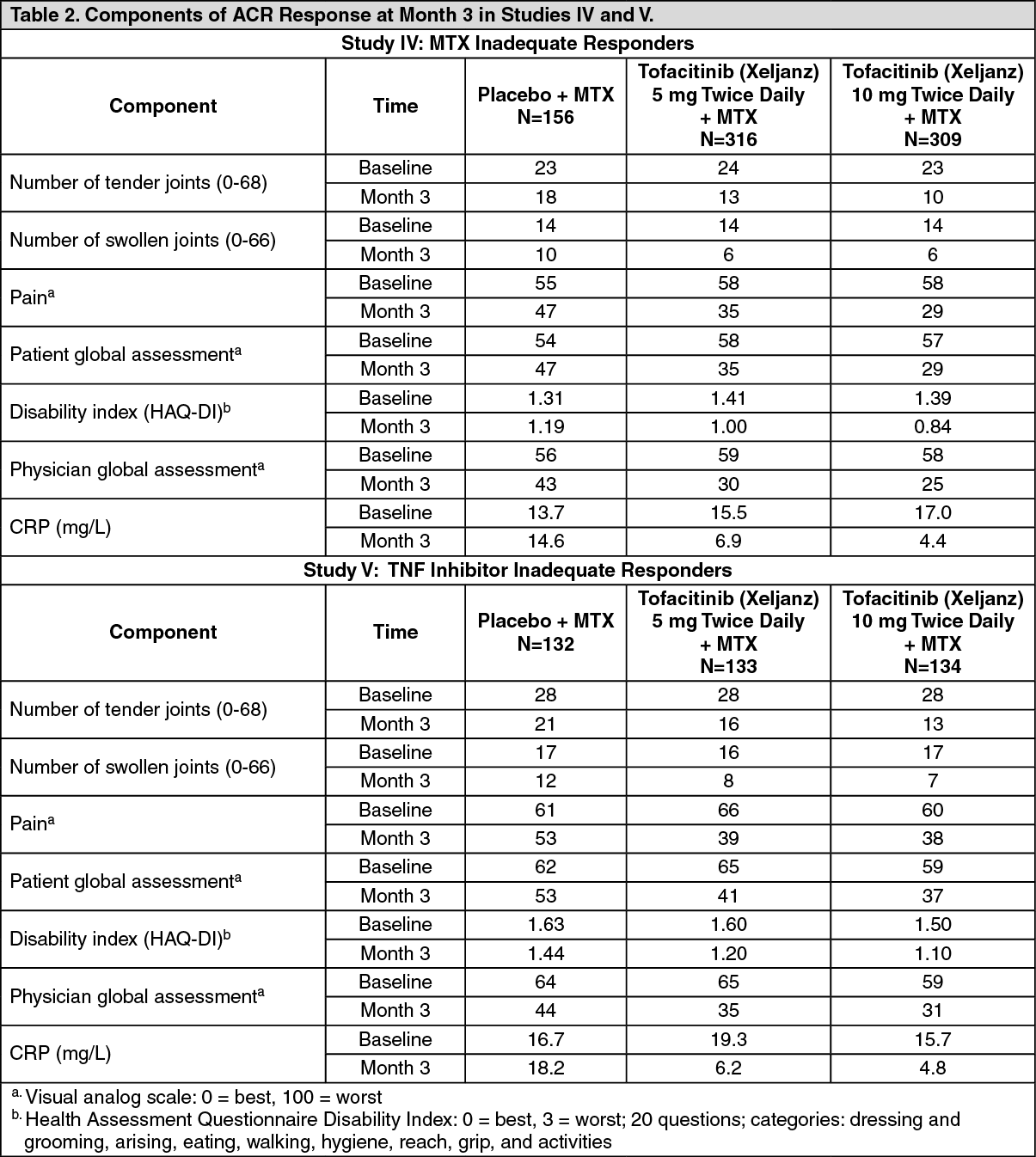 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image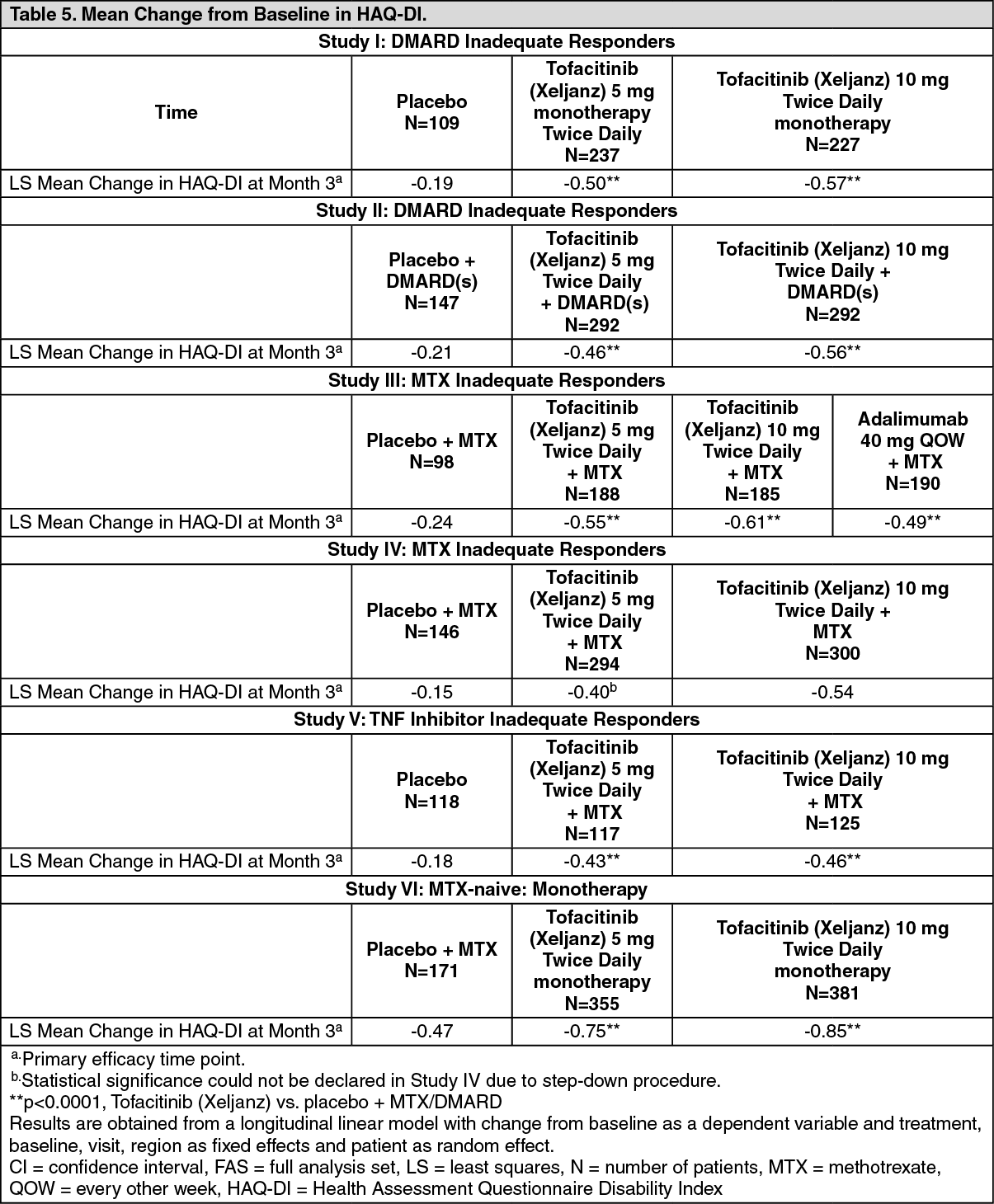 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image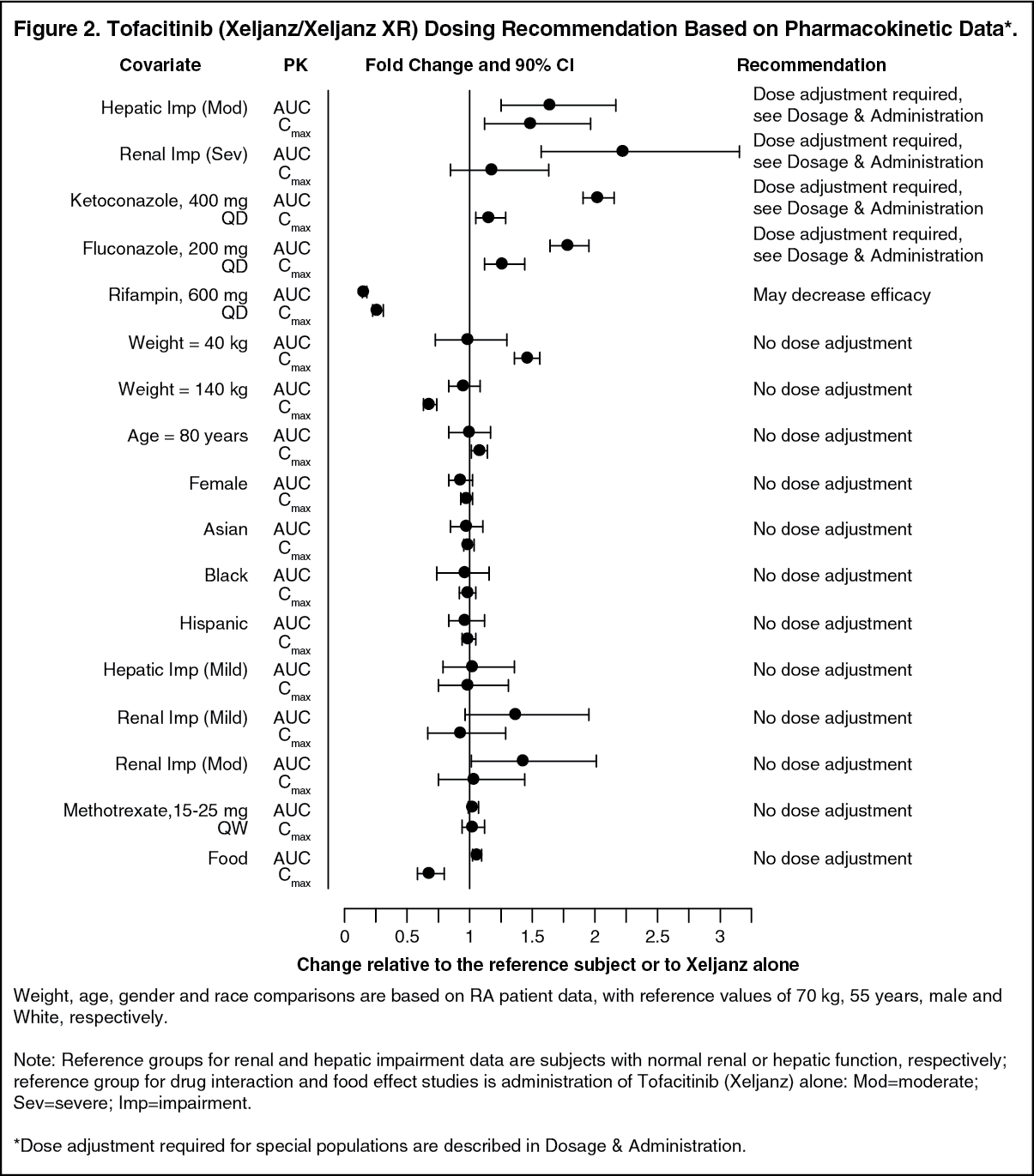 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
